
Anterior knee pain
Anterior knee pain, what is it and what can we do about it?
If you have ever felt a dull, aching pain behind or around your kneecap while running, tackling a flight of stairs, or squatting down, you are far from alone. This condition—Patellofemoral Pain (PFP), Anterior Knee Pain (AKP) or Patellofemoral Pain Syndrome (PFPS), is incredibly common in both active and less active individuals
Historically, treating PFP has been a bit of a guessing game, leading to a frustrating reality: over 50% of people still report persistent knee issues five years after their diagnosis.
Fortunately, a major new study has completely changed the game for treating this condition. By looking at data from thousands of patients and teaming up with real people and top knee experts, researchers have created the ultimate, modern recovery guide. It balances hard science with what patients actually need, giving us a clear framework for treating this condition and getting back to what you love.
Treatment needs to look at 3 areas to be successful;
1. The Foundation: Education and Listening First
One of the most important takeaways from the modern best-practice guidelines isn't an exercise at all—it's education.
When researchers interviewed real patients, they discovered a common thread: people with runner's knee feel incredibly frustrated when they don't get a clear diagnosis or understand why they are hurting. Furthermore, PFP can take a psychological toll—people with chronic knee pain are statistically six times more likely to struggle with anxiety or depression.
The Golden Rule of Best Practice
Before picking up a single weight, a clinician must perform a thorough assessment to understand your unique risk factors, daily habits, and goals. Rehab shouldn't feel like a cookie-cutter checklist; it should begin with a clear explanation of what is happening under your kneecap and how your recovery plan will address it.
2. The Core Intervention: Heavy on the Knee, Helpful on the Hip
Exercise therapy is the cornerstone of effective treatment for this condition, you need to get the knee moving. this can be challenging but with the correct plan and support you will get an effective rehab plan in place.
However, the modern guide narrows the target area specifically to:
Knee-Targeted Exercise: Re-building strength in the quadriceps (the thigh muscles) is the highest-ranked and most recommended intervention. This involves progressive load training, using both non-weight-bearing movements (like knee extensions) and weight-bearing movements (like controlled squats).
Hip-Targeted Exercise: Combined hip-and-knee training is highly effective. Strengthening your glutes and hip posterolateral musculature helps better stabilize the entire lower limb, taking the mechanical stress off your patellofemoral joint.
When starting in rehab, your routine to 3 or 4 high-quality exercises at a time. This will avoid overloading the knee, help build confidence in using it again and most importantly avoiding flaring symptoms.
.
3. The Supporting Cast: Tailored Adjunct Therapies
Every knee is different. Once the foundation of education and exercise is laid, the best practice guide recommends layering in specific "supportive" treatments. Crucially, these shouldn't be used instead of exercise, but rather alongside it to manage immediate pain.
The study identified four supportive interventions backed by clinical agreement:
Foot Orthoses: Ready made shoe inserts can change the alignment of your stride and take immediate pressure off the knee, especially if you have highly mobile feet or pronate heavily.
Manual Therapy: Hands-on physical therapy can help improve joint and tissue mobility, particularly around the ankle or lateral structures of the knee.
Movement & Running Retraining: Modifying your biomechanics (such as slightly increasing your running cadence) can shift the mechanical load away from the kneecap.
Patellar Taping Techniques: These can provide brilliant short-term pain relief, helping you get through your rehab exercises comfortably.
According to the guide, passive modalities such as dry needling, vibration therapy, and hyaluronic acid injections were classified as not effective for patellofemoral pain. Ultrasound and basic electrical stimulation also fell off the recommended list. If your therapy routine relies strictly on you lying passively on a table while a machine does the work, it’s time to rethink your strategy.
The challenge with getting started with effective treatment is getting the right diagnosis in the first place, This is where seeing an experienced physiotherapist is essential. They can perform an effective assessment and examination. This will be important as there are lots of reasons for getting anterior knee pain.
https://www.researchgate.net/publication/384913179_Best_practice_guide_for_patellofemoral_pain_based_on_synthesis_of_a_systematic_review_the_patient_voice_and_expert_clinical_reasoning#:~:text=INTRODUCTION,of%20people%20reporting%20persistent%20pain.
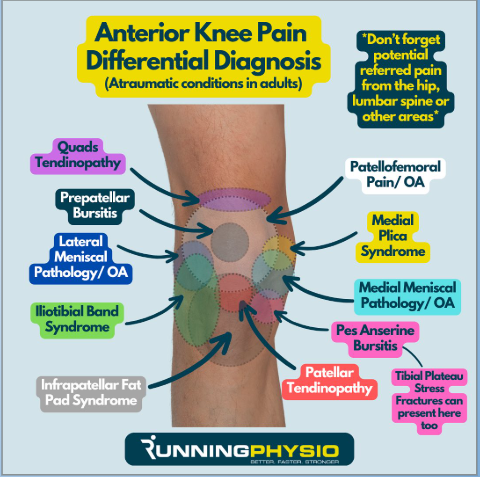
I really like this image from Tom Goom (The Running Physio). It shows nicely how complex pain at the front of the knee can be. each one will have its own history, specifics about the issues it gives a person and each will need a different management strategy. These isn't a one size fits all treatment plan for these conditions.
If you are experiencing pain at the front of the knee and would like a detailed assessment and tailored treatment plan use the link below to book in for an appointment or contact us to discuss how we will be able to help. Our goal will be to use evidence and a quality assessment to build a rehab plan that suits your needs and lifestyle to help you recover and perform.



