A Real Pain in the... Inguinal
Adductor Related Groin Pain
Late 20's female who complained of 4 month history of intermittent groin pain after increasing her training at CrossFit. Main problems were heavy squats, wall balls and running. She had tried resting and some sports massage but the issue persisted. There was no report of back or hip pain or a history of hip pain, no pins and needles or numbness. On examination she had excellent range of motion in the hip and was able to fully squat - this did reveal excessive hip flexion, all pain free. Isometric hold using her adductors reproduced the pain and there was tenderness at the muscle tendon junction of her adductor magnus. Testing also revealed weakness in control of her trunk and pelvis along with weakness in hip extension and abduction. Pain limited her strength in adduction. There was no muscle tightness. She was suffering with adductor related groin pain (ARGP).
A rehab plan was set up to allow continued training, albeit with some activity modifications to avoid exacerbating her pain. A graded loading programme was put in place to target her adductor complex along with lots of education and reassurance on the nature of the problem.
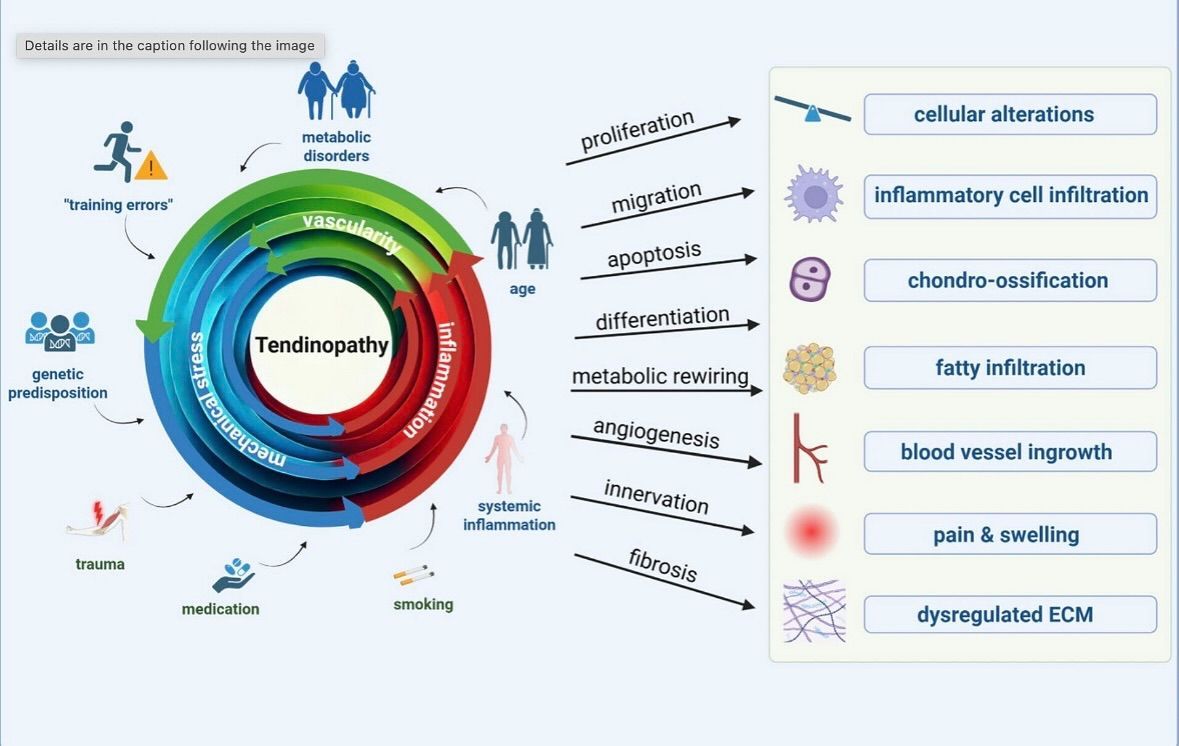
This nice illustration from @derek_griffin_phd that highlights the factors that can contribute to developing a tendinopathy. It will exist on a continuum from acute to chronic. The tendon continuum model describes how your tendons respond to stress across three overlapping stages: Reactive, Dysrepair, and Degenerative.
The Three Stages of Tendon Health
Reactive Tendinopathy: Think of this as a "flare-up." It usually happens after a sudden burst of unaccustomed activity (like a new workout or a sudden increase in running miles). The tendon thickens slightly to protect itself from the load; it’s painful and swollen, but the structure is still intact and can fully return to normal with a short period of rest and modified activity.
Tendon Dysrepair: If the tendon continues to be overloaded without enough rest, it moves into "failed healing." The internal structure becomes more disorganized, and the body may start growing extra blood vessels and nerves in the area to try to fix it, making the tendon more sensitive.
Degenerative Tendinopathy: This is the chronic stage often seen in older athletes or those with long-term injuries. Large portions of the tendon's fibres are now broken down or "silent," meaning they can no longer handle weight effectively. While these damaged areas may not fully heal, the healthy parts around them can still be strengthened. This summed up nicely here https://bjsm.bmj.com/content/50/19/1187 by Cook et al (2016).
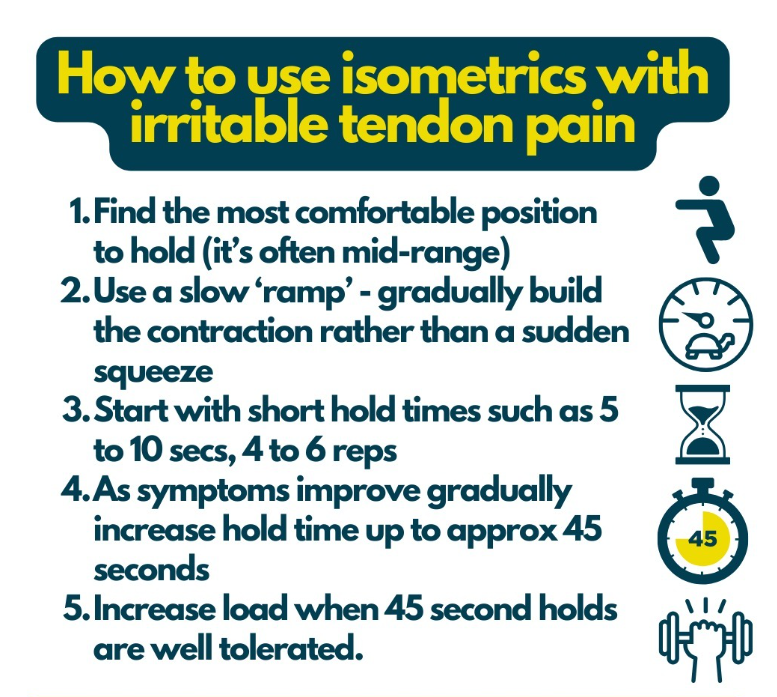
The next challenge is knowing how to address it. In essence the aim is to build resilience and capacity within the tendon to tolerate higher loads through range and with greater rates of force development. The challenge is often finding the appropriate starting point and increasing loading variables but taking account of the tendon response to the new stimulus.
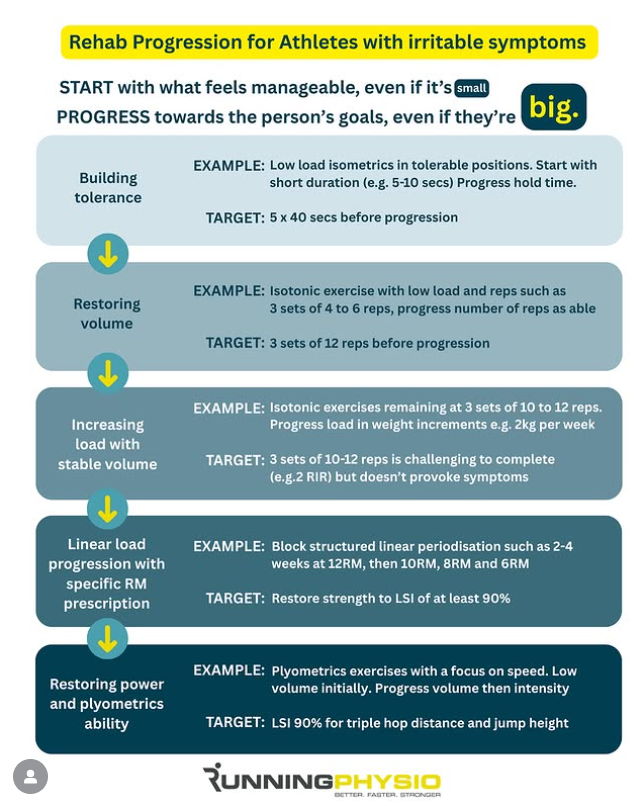
We were able to start with low level isometrics in a comfortable mid range progression along with core strengthening and hip extension and abduction work to address some of the imbalances found on testing. Loading duration and intensity was increased along with more challenging positions in the coming months and exposure to previously problematic movements and actions (depth of squat and a graded running programme with a focus on distance and speed).
The graphic shown opposite is a great starting point from @clinicaledge for tendon loading across the spectrum. Frequency of loading is also important with consistency of work and rest days in a ratio 1:1 or 1:2.